- Introduction: Understanding the Pathology
SPG4 is the most prevalent form of Hereditary Spastic Paraplegia (HSP), accounting for approximately 40% of all autosomal dominant cases. It is a slow-onset, neurodegenerative condition that primarily targets the upper motor neurons. Unlike many other neurological disorders, SPG4 is typically “pure,” meaning it focuses almost exclusively on lower-limb spasticity and weakness without affecting cognitive function or the upper body in most patients. - Genetic and Cellular Mechanisms
At the heart of SPG4 is a mutation in the SPAST gene, which encodes the protein Spastin.
The Role of Spastin: Spastin is an enzyme (an ATPase) responsible for “severing” microtubules. Think of microtubules as the structural scaffolding and “railway tracks” inside a nerve cell.
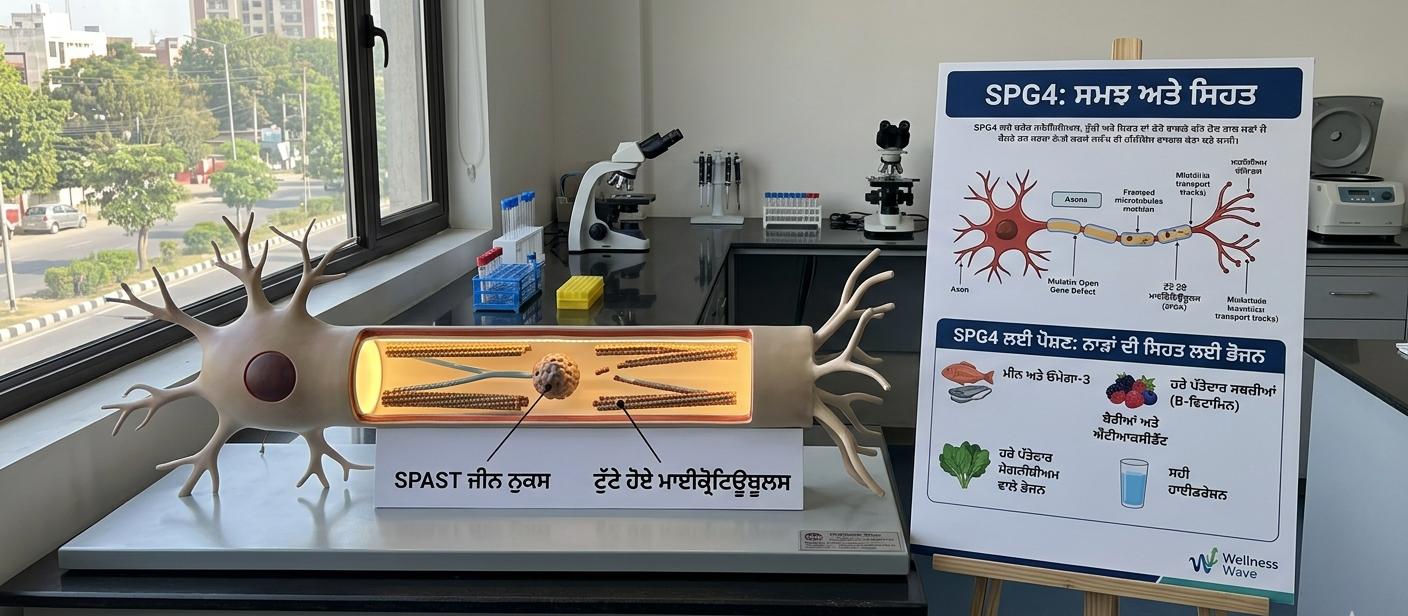
The Breakdown: When the SPAST gene is mutated, Spastin cannot regulate these tracks. This leads to a traffic jam of cellular components. Since the motor neurons traveling from the brain to the legs are the longest cells in the body (sometimes over a meter long), they are the most vulnerable to these transport failures.
Axonal Degeneration: Over time, the ends of these long nerves (axons) begin to “wither” or degenerate, leading to the loss of muscle control.
- Clinical Manifestations (Symptoms)
Symptoms usually emerge insidiously. While it can appear in childhood, the peak onset is during the second to fourth decades of life.
Motor Symptoms
Lower Limb Spasticity: Persistent muscle stiffness, particularly in the hamstrings, calves, and adductors.
Progressive Weakness: Difficulty in “dorsiflexion” (lifting the toes), leading to frequent tripping.
Scissoring Gait: A walking pattern where the legs tend to cross over each other due to tight inner-thigh muscles.
Clonus: Involuntary, rhythmic muscle contractions, often triggered by stretching the ankle.
Non-Motor Symptoms
Urinary Urgency: An overactive bladder caused by spasticity in the muscles governing the urinary tract.
Diminished Vibration Sense: A subtle loss of sensation in the feet, often detected during clinical exams.
- Diagnostic Pathway
Clinical Evaluation: A neurologist assesses reflexes (looking for hyperreflexia) and muscle tone.
Genetic Testing: The “Gold Standard.” Sequencing the SPAST gene can confirm the diagnosis in the majority of cases.
Differential Diagnosis: MRI of the brain and spine is performed to rule out Multiple Sclerosis (MS), Vitamin B12 deficiency, or spinal tumors.
- Specialized Nutrition for SPG4
As a nutritionist, you know that while diet cannot “fix” a genetic mutation, it can significantly alter the neuro-inflammatory environment and support axonal health. Recent research highlights a correlation between lower muscle mass and higher disease severity in HSP patients.
A. The “Neuro-Protective” Macronutrient Profile
High-Quality Protein (1.2–1.5g per kg of body weight): To combat the muscle wasting associated with SPG4, a higher protein intake is required. Focus on branched-chain amino acids (BCAAs) found in lean poultry, fish, and plant proteins like tempeh and lentils.
Anti-Inflammatory Fats: Chronic spasticity creates systemic stress. Focus on Omega-3 fatty acids (EPA and DHA) from fatty fish, walnuts, and flaxseeds to stabilize neuronal membranes.
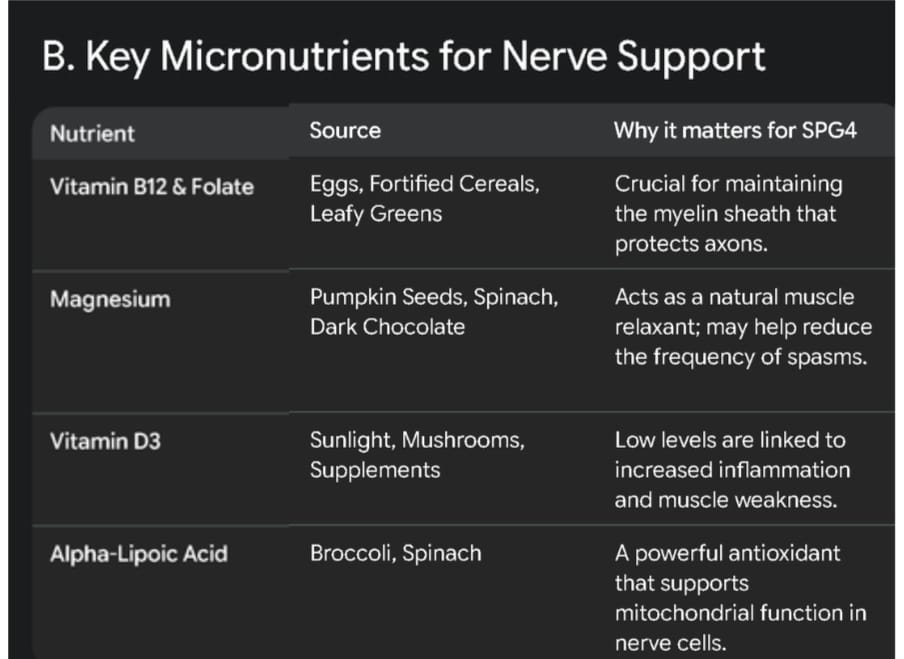
B. Key Micronutrients for Nerve Support
C. Metabolic Management
Evidence suggests that obesity significantly worsens the prognosis of SPG4 by increasing the mechanical load on already weakened lower limbs.
Low-Glycemic Index (GI) Diet: Prevents insulin spikes that can exacerbate neuro-inflammation.
Fiber Intake: High fiber is essential to prevent constipation, a common side effect of both the disease (reduced mobility) and the medications (like Baclofen).
- Multidisciplinary Management
Physical and Occupational Therapy
Stretching Protocol: Twice-daily stretching of the Achilles tendon and hamstrings is mandatory to prevent permanent “contractures” (shortening of the muscles).
Hydrotherapy: Warm water (30–32°C) exercises are the most effective way to improve range of motion without the risk of falls.
Pharmacological Intervention
Muscle Relaxants: Baclofen and Tizanidine are standard.
Botulinum Toxin (Botox): Targeted injections for specific muscle groups that are severely spastic.
- Prognosis and Outlook
SPG4 is not a life-limiting condition. Life expectancy is typically normal. The goal of modern medicine is to move from “symptom management” to “cellular repair.” Emerging research in Gene Therapy aims to deliver healthy SPAST genes directly to the neurons, though this remains in the clinical trial phase.
Nutritionist’s Summary Table for Patients
DO: Prioritize hydration (2-3L water/day), Magnesium-rich foods, and lean proteins.
LIMIT: Pro-inflammatory triggers like refined sugars, trans-fats (processed snacks), and excessive caffeine.
MONITOR: Check Vitamin D and B12 levels every 6 months .
Health Desk
Sandeep Dhand
Nutritionist And Health Educator